Employee COVID-19 Self-Assessment Guideline Summaries
Employee COVID-19 Self-Assessment Guideline Summaries
Employee COVID-19 Self-Assessment Guideline Summaries
States all over the U.S. and provinces in Canada are enforcing different COVID-19 workplace guidelines and requirements for reopening businesses and restarting their economies. One of the most common requirements is that employers implement procedures for screening their employees for COVID-19 symptoms prior to reporting to work. This COVID-19 screening app for employees reduces the spread of COVID-19 and helps keep employees safe. You can find more details about your specific region's employee pre-shift screening requirements below.
Below you can find links to summaries of the requirements for states in the U.S. and provinces in Canada, including temperature recording requirements, and travel restrictions.

U.S. State Employee Symptom Screening Requirements
ALtogether Alabama:
It is strongly recommended that all businesses follow applicable covid-19-related safety guidelines from the Food and Drug Administration and the Centers for Disease Control and Prevention (CDC) publication, Reopening Guidance for Cleaning and Disinfecting Public Spaces, Workplaces, Businesses, Schools, and Homes, at https://www.cdc.gov/coronavirus/2019-ncov/community/reopen-guidance.html
State Questionnaire:
Have you been in close contact with a confirmed case of COVID-19?
Are you experiencing a cough, shortness of breath or sore throat?
Have you had a fever in the last 48 hours?
Have you experienced new loss of taste or smell?
Have you experienced vomiting or diarrhea in the last 24 hours?
Additional information:
Guidelines For Safeguarding All BusinessesGovernor's Website
ALtogether Alabama Start for Free
Reopen Alaska Responsibly:
There are a number of strategies and actions that individuals, businesses, and communities can take to help reduce the spread of the virus that causes COVID-19. This document outlines these strategies and provides resources Alaskans can use to keep themselves, their families, and their communities safe. Alaskans have a proud history of taking care of themselves and their communities during difficult times – Alaska wins when we work together.
Core practices that should remain in place once facilities begin to reopen include:
- Have a staff management plan that includes non-punitive and flexible sick leave policies, staffing patterns in case of restrictions or shortage, and pre-shift screening
State Questionnaire:
Have you had any of the following COVID-19 symptoms since your last day at work or the last time you were here:
- Fever (100.4F or higher) or chills?
- Cough?
- Shortness of breath or difficulty breathing?
- Fatigue?
- Muscle or body aches?
- Headache?
- New loss of taste or smell?
- Sore throat?
- Congestion or runny nose?
- Nausea or vomiting?
- Diarrhea?
- Persistent pain or pressure in the chest?
- New confusion?
- Inability to wake or stay awake?
- Bluish lips or face?
Additional information:
Reopen Alaska ResponsiblyPhase 3/4 General Guidance
Phase 3/4 Detailed Guidance Start for Free
Arizona Together
Stay Healthy. Return Smarter. Return Stronger.
Requirements for Preventing COVID-19 Transmission
Pursuant to the previous and updated guidance issued by the Centers for Disease Control and Prevention (CDC) and the Arizona Department of Health Services (ADHS), under all circumstances, the following precautions are required for businesses operating in Arizona:
- Implement symptom screening for employees prior to the start of their shift.
- Wellness/symptom checks, including temperature checks for all personnel, when possible, as they arrive on premises or before opening.
- Health checks should be done in a private location to avoid stigma and discrimination in the workplace. Information should be kept confidential.
State Questionnaire:
Have you had any of the following COVID-19 symptoms since your last day at work or the last time you were here:
- Fever (100.4F or higher) or chills?
- Cough?
- Shortness of breath or difficulty breathing?
- Fatigue?
- Muscle or body aches?
- Headache?
- New loss of taste or smell?
- Sore throat?
- Congestion or runny nose?
- Nausea or vomiting?
- Diarrhea?
- Persistent pain or pressure in the chest?
- New confusion?
- Inability to wake or stay awake?
- Bluish lips or face?
Additional information:
Arizona General Reopening GuidanceRequirements for Businesses
Barber and Cosemetologist Guidelines
Restaurant Guidelines
Gym and Fitness Provider Guidelines
Retail Guidelines
Spa and Massage Therapy Guidelines
Shopping Mall Guidelines
Theater Guidelines
Casino Guidelines
Start for Free
Arkansas Department of Health
The Secretary of Health has issued this Directive in conjunction with Executive Order 20-25, which imposed limitations on businesses in the state of Arkansas to limit the spread of COVID-19. This directive to include the following steps thatmust be taken to protect the people of the State of Arkansas from COVID-19.
All businesses, manufacturers, and construction companies must implement the following protocols for diminishing the threat of COVID-19:
- Employees should be screened for fever, cough, shortness of breath, sore throat, or loss of taste or smell as they are entering the building at the beginning work.
State Questionnaire:
Have you had any of the following COVID-19 symptoms since your last day at work or the last time you were here:
- Fever (100.4F or higher) or chills?
- Cough?
- Shortness of breath or difficulty breathing?
- Fatigue?
- Muscle or body aches?
- Headache?
- New loss of taste or smell?
- Sore throat?
- Congestion or runny nose?
- Nausea or vomiting?
- Diarrhea?
- Persistent pain or pressure in the chest?
- New confusion?
- Inability to wake or stay awake?
- Bluish lips or face?
Resilence Road Map Phase 2 (May 14, 2020):
Before reopening, all facilities must:
Train employees on how to limit the spread of COVID-19, including how to screen themselves for symptoms and stay home if they have them
Implement individual control measures and screenings
State Questionnaire:
Have you had any of the following COVID-19 symptoms since your last day at work or the last time you were here:
- Fever (100.4F or higher) or chills?
- Cough?
- Shortness of breath or difficulty breathing?
- Fatigue?
- Muscle or body aches?
- Headache?
- New loss of taste or smell?
- Sore throat?
- Congestion or runny nose?
- Nausea or vomiting?
- Diarrhea?
- Persistent pain or pressure in the chest?
- New confusion?
- Inability to wake or stay awake?
- Bluish lips or face?
Additional information:
California's Industry Guidance to Reduce RiskResilience Roadmap
Start for Free
Safer At Home
Second Amended Public Health Order 20-28
Employers with over fifty (50) employees in any one location shall implement the following protocols:
- implement employee screening systems in one of the following ways:
- Set up stations at the worksite for symptom screening and temperature checks; or
- Create a business policy that requires at-home employee self-screening each work day and reporting of the results to the employer prior to entering the worksite;
State Questionnaire:
Have you had any of the following COVID-19 symptoms since your last day at work or the last time you were here:
- Fever (100.4F or higher) or chills?
- Cough?
- Shortness of breath or difficulty breathing?
- Fatigue?
- Muscle or body aches?
- Headache?
- New loss of taste or smell?
- Sore throat?
- Congestion or runny nose?
- Nausea or vomiting?
- Diarrhea?
- Persistent pain or pressure in the chest?
- New confusion?
- Inability to wake or stay awake?
- Bluish lips or face?
Reopen Connecticut:
Daily Health Check
Ask employees resuming on-premise work to confirm they have not experienced COVID-19 CDC-defined symptoms and to monitor their own symptoms, including cough, shortness of breath, or any two of the following symptoms:
Fever
Chills
Repeated shaking with chills
Muscle Pain
Headache
Sore throat
New loss of taste or smell
State Questionnaire:
Have you had any of the following COVID-19 symptoms since your last day at work or the last time you were here:
- Fever (100.4F or higher) or chills?
- Cough?
- Shortness of breath or difficulty breathing?
- Fatigue?
- Muscle or body aches?
- Headache?
- New loss of taste or smell?
- Sore throat?
- Congestion or runny nose?
- Nausea or vomiting?
- Diarrhea?
- Persistent pain or pressure in the chest?
- New confusion?
- Inability to wake or stay awake?
- Bluish lips or face?
Additional information:
Documents containing the rules for the first phase of reopening have been published on the state’s coronavirus website – ct.gov/coronavirus– and are available to download directly at these links:
For more information visit: Connecticut's Rules for Businesses Under First Phase of Reopening Plans
Start for FreeDelaware's Economic Reopening:
All employees required to go to work should perform a daily health check as prescribed by the Delaware Division of Public Health.
Delaware Division of Public Health's Screening Recommendations:
Employers must screen each incoming employee with a basic questionnaire, which should include at least the below, however can be made more comprehensive and/or employer-specific in consultation with medical professionals
- Do you have symptoms of respiratory infection (feveror shaking chills, cough, shortness of breath, severe sore throat, loss of taste or smell, or muscle aches)?
- Have you been in close contact(e.g., within 6 feet for more than 10minutes) with a person with confirmed COVID-19 infection?
State Questionnaire:
- Do you have symptoms of respiratory infection (feveror shaking chills, cough, shortness of breath, severe sore throat, loss of taste or smell, or muscle aches)?
- Do your symptoms have a known cause (asthma, COPD, chronic sinusitis, etc.)?
- Have you been in close contact(e.g., within 6 feet for more than 10 minutes) with a person with confirmed COVID-19 infection?
Florida's Plan for Recovery:
Consider conducting daily in-person or virtual health checks (e.g., symptom and/or temperature screening) of employees before they enter the facility, in accordance with state and local public health authorities and, if available, your occupational health services:
State Questionnaire:
Have you had any of the following COVID-19 symptoms since your last day at work or the last time you were here:
- Fever (100.4F or higher) or chills?
- Cough?
- Shortness of breath or difficulty breathing?
- Fatigue?
- Muscle or body aches?
- Headache?
- New loss of taste or smell?
- Sore throat?
- Congestion or runny nose?
- Nausea or vomiting?
- Diarrhea?
- Persistent pain or pressure in the chest?
- New confusion?
- Inability to wake or stay awake?
- Bluish lips or face?
Additional information:
Florida's Guidelines for Businesses and EmployersCDC Guidelines for Employers
Start for Free
Reviving A Healthy Georgia:
All Restaurants, Dining Rooms, and non-critical businesses that continue in-person operations during the effective dates of this order shall implement measures wheich mitigate the exposure and spread of COVID-19 among its workforce. Such measures shall include the following:
- Screening and evaluating Workers who exhibit symptoms of COVID-19
Critical Infrastructure that continue in-person operation during the effective dates of this order shall implement measures which mitigate the exposure and spread of COVID-19. Such measures may include, byt shall not be limited to the following, which shall be implemented to the maximum extent practicable:
- Screening and evaluating Workers who exhibit symptoms of COVID-19
State Questionnaire:
Have you had any of the following COVID-19 symptoms since your last day at work or the last time you were here:
- Fever (100.4F or higher) or chills?
- Cough?
- Shortness of breath or difficulty breathing?
- Fatigue?
- Muscle or body aches?
- Headache?
- New loss of taste or smell?
- Sore throat?
- Congestion or runny nose?
- Nausea or vomiting?
- Diarrhea?
- Persistent pain or pressure in the chest?
- New confusion?
- Inability to wake or stay awake?
- Bluish lips or face?
Hawaii's Roadmap to Recovery and Resilience
Restaurants for Dine-In Service, Retail Food Markets, Food Processors & Manufacturers:
Before starting their shift, all staff should be screened and evaluated for signs of illness.
State Questionnaire:
Have you had any of the following COVID-19 symptoms since your last day at work or the last time you were here:
- Fever (100.4F or higher) or chills?
- Cough?
- Shortness of breath or difficulty breathing?
- Fatigue?
- Muscle or body aches?
- Headache?
- New loss of taste or smell?
- Sore throat?
- Congestion or runny nose?
- Nausea or vomiting?
- Diarrhea?
- Persistent pain or pressure in the chest?
- New confusion?
- Inability to wake or stay awake?
- Bluish lips or face?
Additional information:
Hawaii's COVID-19 PageGuidance for Reopening Food Services Sector
Start for Free
Idaho Rebounds: Our Path to Prosperity
Governor Brad Little, with the help of the Department of Health and Welfare and guidance issued by President Donald Trump and the Centers for Disease Control and Prevention, has established a data-driven approach to opening up Idaho’s economy. This approach reduces the risk of COVID-19 to Idaho’s most vulnerable populations and preserves capacity in our healthcare system, while opening up businesses safely. From an economic standpoint, Idaho’s rebound from COVID-19 starts with employee and consumer confidence, which leads into business stability and growth and eventually promotion and attraction.
General Businesses:
On a case-by-case basis, include other practices such as screening of employees for illness and exposures upon work entry, requiring non-cash transactions, etc.
Restaurants:
Monitor employee health by screening employees for fever and symptoms before every shift
State Questionnaire:
Have you had any of the following COVID-19 symptoms since your last day at work or the last time you were here:
- Fever (100.4F or higher) or chills?
- Cough?
- Shortness of breath or difficulty breathing?
- Fatigue?
- Muscle or body aches?
- Headache?
- New loss of taste or smell?
- Sore throat?
- Congestion or runny nose?
- Nausea or vomiting?
- Diarrhea?
- Persistent pain or pressure in the chest?
- New confusion?
- Inability to wake or stay awake?
- Bluish lips or face?
Additional information:
Stages of ReopeningBusiness Specific Protocols for Reopening
Start for Free
Restore Illinois: A Public Health Approach to Safely Reopen our State
Restore Illinois is about saving lives and livelihoods. This five-phased plan will reopen our state, guided by health metrics and with distinct business, education, and recreation activities characterizing each phase. This is an initial framework that will likely be updated as research and science develop and as the potential for treatments or vaccines is realized. The plan is based upon regional healthcare availability, and it recognizes the distinct impact COVID-19 has had on different regions of our state as well as regional variations in hospital capacity.
All employers should have a wellness screening program. Resources outlining screening program best practices are posted on the DCEO Restore Illinois guidelines website.
-
Employers should conduct in-person screening of employees upon entry into workplace and mid-shift screening to verify no presence of COVID-19 symptoms;
State Questionnaire:
Employers may ask employees to respond “Yes” or “No” to each question below OR show a list of symptoms to employees and ask them to answer whether or not they are experiencing any of them.
- Have you felt feverish?
- Do you have a cough?
- Do you have a sore throat?
- Have you been experiencing difficulty breathing or a shortness of breath?
- Do you have muscle aches?
- Have you had a new or unusual headache (e.g., not related to caffeine, diet, or hunger, not related to a history of migraines, clusters, or tension, not typical to the individual)?
- Have you noticed a new loss of taste or loss of smell?
- Have you been experiencing chills or rigors?
- Do you have any gastrointestinal concerns (e.g., abdominal, pain, vomiting, diarrhea)?
- Is anyone in your household displaying any symptoms of COVID-19?
- To the best of your knowledge, have you or anyone in your household come into close contact with anyone who has tested positive for COVID-19?
Back On Track Indiana:
Employee Screening Procedures– Conduct daily health assessments by utilizing a screening procedure for COVID-19 symptoms for employees who are reporting for work. Examples include self-assessments before arrival in the workplace, screening questions, or taking temperatures with a no-touch thermometer
State Questionnaire:
Have you had any of the following COVID-19 symptoms since your last day at work or the last time you were here:
- Fever (100.4F or higher) or chills?
- Cough?
- Shortness of breath or difficulty breathing?
- Fatigue?
- Muscle or body aches?
- Headache?
- New loss of taste or smell?
- Sore throat?
- Congestion or runny nose?
- Nausea or vomiting?
- Diarrhea?
- Persistent pain or pressure in the chest?
- New confusion?
- Inability to wake or stay awake?
- Bluish lips or face?
Reopening Iowa
Workplaces, particularly in areas where community transmission of COVID-19 is occurring, should consider developing and implementing a comprehensive screening and monitoring strategy aimed at preventing the introduction of COVID-19 into the work site. Consider a program of screening workers before entry into the workplace, criteria for exclusion of sick workers, including asymptomatic workers who have tested positive for COVID-19; and criteria for return to work of exposed and recovered (those who have had signs or symptoms of COVID-19 but have gotten better).. This type of program should be coordinated to the extent possible with local public health authorities
State Questionnaire:
Have you had any of the following COVID-19 symptoms since your last day at work or the last time you were here:
- Fever (100.4F or higher) or chills?
- Cough?
- Shortness of breath or difficulty breathing?
- Fatigue?
- Muscle or body aches?
- Headache?
- New loss of taste or smell?
- Sore throat?
- Congestion or runny nose?
- Nausea or vomiting?
- Diarrhea?
- Persistent pain or pressure in the chest?
- New confusion?
- Inability to wake or stay awake?
- Bluish lips or face?
Additional information:
Iowa Department of Public HealthCDC Employee Screening Guidelines
Start for Free
Ad Astra: A Plan to Reopen Kansas
Protect Your Team
Monitor employees temperatures and symptoms regularly. Issue or approve face coverings. Be mindful of spaces where 6 feet of distance can’t be maintained. Disinfect workspaces at the beginning and end of each shift/work day.
State Questionnaire:
Have you had any of the following COVID-19 symptoms since your last day at work or the last time you were here:
- Fever (100.4F or higher) or chills?
- Cough?
- Shortness of breath or difficulty breathing?
- Fatigue?
- Muscle or body aches?
- Headache?
- New loss of taste or smell?
- Sore throat?
- Congestion or runny nose?
- Nausea or vomiting?
- Diarrhea?
- Persistent pain or pressure in the chest?
- New confusion?
- Inability to wake or stay awake?
- Bluish lips or face?
Additional information:
Reopening PlanAd Astra Website
Business Guidelines
Department of Health Recommendations
Start for Free
Kentucky Healthy at Work:
Daily temperature and health checks may be administered by the employer at the business site or self-administered by the employee prior to arriving at work (at least once every 24-hour period).
State Questionnaire:
Have you had any of the following COVID-19 symptoms since your last day at work or the last time you were here:
- Fever (100.4F or higher) or chills?
- Cough?
- Shortness of breath or difficulty breathing?
- Fatigue?
- Muscle or body aches?
- Headache?
- New loss of taste or smell?
- Sore throat?
- Congestion or runny nose?
- Nausea or vomiting?
- Diarrhea?
- Persistent pain or pressure in the chest?
- New confusion?
- Inability to wake or stay awake?
- Bluish lips or face?
Is there anyone in your household who is showing COVID-19 symptoms or who has been diagnosed with COVID-19?
Have you been in close contact with anyone exhibiting sign or symptoms of fever, persistent cough or shortness of breath consistent with COVID-19 who has not been tested or is still awaiting testing?
Reopening Louisiana
Workplaces, particularly in areas where community transmission of COVID-19 is occurring, should consider developing and implementing a comprehensive screening and monitoring strategy aimed at preventing the introduction of COVID-19 into the work site. Consider a program of screening workers before entry into the workplace, criteria for exclusion of sick workers, including asymptomatic workers who have tested positive for COVID-19; and criteria for return to work of exposed and recovered (those who have had signs or symptoms of COVID-19 but have gotten better).. This type of program should be coordinated to the extent possible with local public health authorities.
State Questionnaire:
Have you had any of the following COVID-19 symptoms since your last day at work or the last time you were here:
- Fever (100.4F or higher) or chills?
- Cough?
- Shortness of breath or difficulty breathing?
- Fatigue?
- Muscle or body aches?
- Headache?
- New loss of taste or smell?
- Sore throat?
- Congestion or runny nose?
- Nausea or vomiting?
- Diarrhea?
- Persistent pain or pressure in the chest?
- New confusion?
- Inability to wake or stay awake?
- Bluish lips or face?
Restarting Maine's Economy
The State of Maine has adopted a staged approach, supported by science, public health expertise, and industry collaboration, to allow Maine businesses to safely open when the time is right.
State Questionnaire:
Ask employees and customers the following questions to screen for illness:
- Have you had a cough or sore throat?
- Have you had a fever or do you feel feverish?
- Do you have shortness of breath?
- Do you have a loss of taste or smell?
- Have you been around anyone exhibiting these symptoms within the past 14 days?
- Are you living with anyone who is sick or quarantined?
- Have you been out of state in the last 14 days?
Additional information:
Restarting Maine's EconomyCOVID19 Prevention Checklist Industry Guidance
Start for Free
Maryland is Back to Business
Maryland is following Governor Hogan’s Maryland Strong: Roadmap to Recovery plan, which includes a phased approach to reopening business. Effective May 15 at 5 p.m., Maryland is in Stage One of recovery, which includes the reopening of some businesses, such as manufacturing, retail stores, and some personal services. Business owners are urged to review Governor Hogan’s Executive Order and Interpretive Guidance for more details on reopening.
For Employers:
- Screen employees for COVID-19 symptoms at start of work.
State Questionnaire:
Have you had any of the following COVID-19 symptoms since your last day at work or the last time you were here:
- Fever (100.4F or higher) or chills?
- Cough?
- Shortness of breath or difficulty breathing?
- Fatigue?
- Muscle or body aches?
- Headache?
- New loss of taste or smell?
- Sore throat?
- Congestion or runny nose?
- Nausea or vomiting?
- Diarrhea?
- Persistent pain or pressure in the chest?
- New confusion?
- Inability to wake or stay awake?
- Bluish lips or face?
Reopening Massachusetts
The Baker-Polito Administration’s comprehensive plan to safely reopen the Massachusetts economy, get people back to work, and ease social restrictions while minimizing the health impacts of COVID-19.
State Questionnaire:
Have you had any of the following COVID-19 symptoms since your last day at work or the last time you were here:
- Fever (100.4F or higher) or chills?
- Cough?
- Shortness of breath or difficulty breathing?
- Fatigue?
- Muscle or body aches?
- Headache?
- New loss of taste or smell?
- Sore throat?
- Congestion or runny nose?
- Nausea or vomiting?
- Diarrhea?
- Persistent pain or pressure in the chest?
- New confusion?
- Inability to wake or stay awake?
- Bluish lips or face?
Additional information:
Reopening MassachusettsMandatory Safety Standards for Workplaces
Start for Free
Michigan: COVID-19 Workplace Guidelines
Employee Screening Procedures - Prior to Work
-
Temperature, self monitoring symptoms (Cough, fever, shortness of breath)
State Questionnaire:
Have you had any of the following COVID-19 symptoms since your last day at work or the last time you were here:
- Fever (100.4F or higher) or chills?
- Cough?
- Shortness of breath or difficulty breathing?
- Fatigue?
- Muscle or body aches?
- Headache?
- New loss of taste or smell?
- Sore throat?
- Congestion or runny nose?
- Nausea or vomiting?
- Diarrhea?
- Persistent pain or pressure in the chest?
- New confusion?
- Inability to wake or stay awake?
- Bluish lips or face?
Minnesota: Safely Returning to Work
Ensure sick workers stay home
- Establish health screening protocols for workers at the start of each shift (e.g. health screening survey, taking temperature). See the Minnesota Department of Health (MDH)’s Visitor and Employee Health Screening Checklist (www.health.state.mn.us/diseases/coronavirus/facilityhlthscreen.pdf). The checklist is also available in Hmong, Somali, and Spanish (www.health.state.mn.us/diseases/coronavirus/businesses.html).
State Questionnaire:
Have you had any of the following symptoms since your last day at work or the last time you were here that you cannot attribute to another health condition?
- Fever or feeling feverish?
- Chills?
- A new cough?
- Shortness of breath?
- A new sore throat?
- New muscle aches?
- New headache?
- New loss of smell or taste?
Safe Return Mississippi
For Businesses:
Businesses and non-profit entities shall take all reasonable measures to ensure compliance with the Mississippi State Department of Health's and CDC's regulations, orders and guidelines to prevent the spread of COVID-19, including, but not limited to, social distancing, sending sick employees home and actively encouraging sick employees to stay home, separating and sending home employees who appear to have respiratory illness symptoms, adopting and enforcing regular and proper hand-washing and personal hygiene protocols and daily screening of employees and volunteers for COVID-19 symptoms before beginning shift.
For Restaurants:
Restaurants and bars shall conduct a daily screening of all employees at the beginning of their shifts. Such daily screening shall include the following questions, and any employee answering any question in the affirmative shall be sent home:
- Have you been in close contact with a confirmed case of COVID-19 in the past 14 days?
- Are you experiencing a cough, shortness of breath, or sore throat?
- Have you had a fever in the last 48 hours?
- Have you had new loss of taste or smell?
- Have you had vomiting or diarrhea in the last 24 hours?
State Questionnaire:
- Have you been in close contact with a confirmed case of COVID-19 in the past 14 days?
- Are you experiencing a cough, shortness of breath, or sore throat?
- Have you had a fever in the last 48 hours?
- Have you had vomiting or diarrhea in the last 24 hours?
Start for Free
Additional information:
Official COVID-19 Updates and ResourcesExecutive Order for Businesses
Executive Order for Restaurants
Show Me Storng
For Businesses:
Develop an infectious disease preparedness and response plan, including policies and procedures for workforce contact tracing when an employee tests positive for COVID-19.
Monitor workforce for indicative symptoms. Do not allow symptomatic people to physically return to work until cleared by a medical provider.
Start for FreeState Questionnaire:
Have you had any of the following COVID-19 symptoms since your last day at work or the last time you were here:
- Fever (100.4F or higher) or chills?
- Cough?
- Shortness of breath or difficulty breathing?
- Fatigue?
- Muscle or body aches?
- Headache?
- New loss of taste or smell?
- Sore throat?
- Congestion or runny nose?
- Nausea or vomiting?
- Diarrhea?
- Persistent pain or pressure in the chest?
- New confusion?
- Inability to wake or stay awake?
- Bluish lips or face?
Additional information:
General Guidelines to Reopen Missouri’s EconomyCDC Employee Screening Guidelines
Montana: Reopening the Big Sky
Guidelines for all Phases: Employers
Develop and implement appropriate policies, in accordance with Federal, State, and local regulations and guidance, and informed by industry best practices, regarding:
- Social distancing and protective equipment.
- Temperature checks and/or symptom screening.
- Collaborate with public health on testing, isolating, and contact tracing.
- Sanitation.
- Use and disinfection of common and high-traffic areas.
Start for Free
State Questionnaire:
Have you had any of the following COVID-19 symptoms since your last day at work or the last time you were here:
- Fever (100.4F or higher) or chills?
- Cough?
- Shortness of breath or difficulty breathing?
- Fatigue?
- Muscle or body aches?
- Headache?
- New loss of taste or smell?
- Sore throat?
- Congestion or runny nose?
- Nausea or vomiting?
- Diarrhea?
- Persistent pain or pressure in the chest?
- New confusion?
- Inability to wake or stay awake?
- Bluish lips or face?
Reopeninig Nebraska
For Restaurants:
complete employee pre-screening (e.g., take temperature and assess for any symptoms consistent with COVID-19) prior to starting work.
For Meat Processing Facilities:
Active Screening
To prevent the transmission of COVID-19in facilities, all employees and essential visitors/contractors should be screened daily.This should include temperature screening as well as screening questions designed to identify individuals with other COVID-19 symptoms or exposure risks. Designated point(s) of entry should be used to facilitate screening of every employee or visitor prior to entry. Visual markers (e.g., tape, spray paint) should be added and spaced out every six feet to prevent workers from crowding during screening process. Provide masks at the earliest possible point during the screening process, ideally prior to screeningand prior toor immediately upon entering the facility.
State Questionnaire:
Have you had any of the following COVID-19 symptoms since your last day at work or the last time you were here:
- Fever (100.4F or higher) or chills?
- Cough?
- Shortness of breath or difficulty breathing?
- Fatigue?
- Muscle or body aches?
- Headache?
- New loss of taste or smell?
- Sore throat?
- Congestion or runny nose?
- Nausea or vomiting?
- Diarrhea?
- Persistent pain or pressure in the chest?
- New confusion?
- Inability to wake or stay awake?
- Bluish lips or face?
Start for Free
Reopeninig Nevada
Mandatory:Employers must perform daily symptom assessment of employees.
Consider conducting daily in-person or virtual health checks (e.g., symptom and/or temperature screening) of employees before they enter the facility, in accordance with state and local public health authorities and, if available, your occupational health services:
Start for FreeState Questionnaire:
Have you had any of the following COVID-19 symptoms since your last day at work or the last time you were here:
- Fever (100.4F or higher) or chills?
- Cough?
- Shortness of breath or difficulty breathing?
- Fatigue?
- Muscle or body aches?
- Headache?
- New loss of taste or smell?
- Sore throat?
- Congestion or runny nose?
- Nausea or vomiting?
- Diarrhea?
- Persistent pain or pressure in the chest?
- New confusion?
- Inability to wake or stay awake?
- Bluish lips or face?
Additional information:
Nevada Health ResponseBusiness and Workforce Guidance
Industry Specific Guidance
New Hampshire: Stay at Home 2.0
Employers must develop a process for screening all employees reporting for work for COVID-19 related symptoms as follows:
- Identify a location and assign a person who will screen each employee every day before they enter the work-place. Such plans should be clearly communicated with employees. The person performing the screening should wear a cloth face covering/mask. All employees (see guidance below) should also wear a cloth face covering while at work and in potential close contact with others.
State Questionnaire:
- Have you been in close contact with a confirmed case of COVID-19?
- Have you had a fever or felt feverish in the last 72 hours?
- Are you experiencing any respiratory symptoms including a runny nose, sore throat, cough, or shortness of breath?
- Are you experiencing any new muscle aches or chills?
- Have you experienced any new change in your sense of taste or smell?
Reopening New Jersey
For Employers with Migrant and Seasonal Farm Workers:
Employer is to screen workers for symptoms, including temperature and symptom checks prior to work shifts.
For Childcare Workers:
Centers will be required to screen children and staff each day, prior to entry into the center. Anyone exhibiting symptoms or with a fever over 100.4 will be prohibited from entering the center.
Start for FreeState Questionnaire:
Have you had any of the following COVID-19 symptoms since your last day at work or the last time you were here:
- Fever (100.4F or higher) or chills?
- Cough?
- Shortness of breath or difficulty breathing?
- Fatigue?
- Muscle or body aches?
- Headache?
- New loss of taste or smell?
- Sore throat?
- Congestion or runny nose?
- Nausea or vomiting?
- Diarrhea?
- Persistent pain or pressure in the chest?
- New confusion?
- Inability to wake or stay awake?
- Bluish lips or face?
Additional information:
New Jersey's COVID-19 Information HubFarm Guidance
Safety Guidlines to Reopen Childcare Centers
Reopening New Mexico
For All Employers:
Required
- Screen employees before they enter the workplace each day (verbally or with a written form or text- based or other app). Send employees home who are experiencing the following COVID-19 symptoms related to COVID-19 and direct them to obtain free testing through the Department of Health.
- Fever
- Cough
- Shortness of breath
- Sore throat
- Headache
- Muscle pain
- Chills
- Repeated shaking with chills
- Loss of taste or smell
State Questionnaire:
Have you had any of the following COVID-19 symptoms since your last day at work or the last time you were here:
- Fever (100.4F or higher) or chills?
- Cough?
- Shortness of breath or difficulty breathing?
- Fatigue?
- Muscle or body aches?
- Headache?
- New loss of taste or smell?
- Sore throat?
- Congestion or runny nose?
- Nausea or vomiting?
- Diarrhea?
- Persistent pain or pressure in the chest?
- New confusion?
- Inability to wake or stay awake?
- Bluish lips or face?
Reopening New York
Implement mandatory health screening assessment (e.g. questionnaire, temperature check) for employees, contractors, and other visitors, asking about (1) COVID-19 symptoms in past 14 days, (2) positive COVID-19 test in past 14 days, and/or (3) close contact with confirmed or suspected COVID-19 case in past 14 days. Responses must be reviewed and documented daily.
Start for FreeState Questionnaire:
Have you knowingly been in close or proximate contact in the past 14 days with anyone who has tested positive for COVID-19 or who has or had symptoms of COVID-19?
Have you tested positive for COVID-19 in the past 14 days?
Have you experienced any symptoms of COVID-19 in the past 14 days?
Besides to and from works, have you traveled to the states that are subjected to self-quarantine within the last two weeks?
North Carolina: Staying Ahead of the Curve
North Carolina is taking a three-phased approach – based on data from testing, tracing and trends and in consultation with members of the business community – to lift restrictions in place to slow the spread of the COVID-19 coronavirus pandemic and save lives.
Easing Restrictions on Travel, Business Operations, And Mass Gatherings: Phase I:
-
Conduct daily symptom screening of workers, using a standard interview questionnaire of symptoms, before workers enter the workplace.
State Questionnaire:
Have you had close contact (within 6 feet for at least 10 minutes) in the last 14 days with someone diagnosed with COVID-19,or has any health department or health care provider been in contact with you and advised you to quarantine?
Since you last worked, have you had any of these symptoms:
- Fever?
- Chills?
- Shortness of breath or difficulty breathing?
- New cough?
- New loss of taste or smell?
Since you last worked, have you been diagnosed with COVID-19?
A worker can return to work when they can answer YES to ALL three questions:
- Has it been at least 10 days since you first had symptoms?
- Has it been at least 3 days since you’ve had a fever (without using fever reducing medicine)?
- Has it been at least 3 days since your symptoms have improved, including cough and shortness of breath?
Additional information:
North Carolina's Phase 1-Easing of RestrictionsExecutive Order
Start for Free
Reopeninig North Dakota
Consider conducting daily in-person or virtual health checks (e.g., symptom and/or temperature screening) of employees before they enter the facility, in accordance with state and local public health authorities and, if available, your occupational health services:
Those who are, or work with, vulnerable populations should undergo daily screening/symptom monitoring and should be tested if they develop symptoms.
Start for FreeState Questionnaire:
Have you had any of the following COVID-19 symptoms since your last day at work or the last time you were here:
- Fever (100.4F or higher) or chills?
- Cough?
- Shortness of breath or difficulty breathing?
- Fatigue?
- Muscle or body aches?
- Headache?
- New loss of taste or smell?
- Sore throat?
- Congestion or runny nose?
- Nausea or vomiting?
- Diarrhea?
- Persistent pain or pressure in the chest?
- New confusion?
- Inability to wake or stay awake?
- Bluish lips or face?
Ohio: Employee Screening for COVID-19
Consider encouraging employees to do a self-assessment each day to check if they have any COVID-19 symptoms (fever, cough, or shortness of breath). For those employees who must report: take your temperature with a thermometer each day. If you have a fever at or above 100.4 degrees Fahrenheit, stay home. Also monitor for coughing and trouble breathing and stay home if they occur. Call a doctor or use telemedicine if your symptoms concern you. Employees can return to work when they meet ALL THREE of the following criteria:
-
They have had NO fever for at least three (3) days without taking medication to reduce fever during that time.
-
There is improvement in their respiratory symptoms (cough and shortness of breath) for three (3) days.
-
At least seven (7) days have passed since their symptoms began.
If you do have symptoms, stay home from work until you meet all of the above criteria:
-
If you do have symptoms, but have a known cause (asthma, COPD, chronic sinusitis, etc.) and HAVE NOT been exposed to someone with confirmed COVID-19 proceed to work.
-
If you do have symptoms, but have a known cause (asthma, COPD, chronic sinusitis, etc.) and HAVE been exposed to someone with confirmed COVID-19, stay home for 14 days from the time you were exposed.
If at any time a doctor confirms the cause of a fever or other symptoms is not COVID-19 and approves an employee’s return to work, then the employee can return.
State Questionnaire:
Have you had NO fever for at least three (3) days without taking medication to reduce fever at that time?
Have you had improvement in respiratory symptoms (cough and shortness of breath) for three (3) days?
Have at least seven (7) days passed since your symptoms began?
If you do have symptoms, do they have a known cause (asthma, COPD, chronic sinusitis, etc.) and have you not been exposed to someone with confirmed COVID-19
If you do have symptoms, has a doctor confirmed it is not COVID-19 and approved your return to work?
Additional information:
Ohio's COVID-19 Information for Employers and EmployeesReopeninig Oklahoma
Consider conducting daily in-person or virtual health checks (e.g., symptom and/or temperature screening) of employees before they enter the facility, in accordance with state and local public health authorities and, if available, your occupational health services:
Start for FreeState Questionnaire:
Have you had any of the following COVID-19 symptoms since your last day at work or the last time you were here:
- Fever (100.4F or higher) or chills?
- Cough?
- Shortness of breath or difficulty breathing?
- Fatigue?
- Muscle or body aches?
- Headache?
- New loss of taste or smell?
- Sore throat?
- Congestion or runny nose?
- Nausea or vomiting?
- Diarrhea?
- Persistent pain or pressure in the chest?
- New confusion?
- Inability to wake or stay awake?
- Bluish lips or face?
Additional information:
Oklahoma's COVID-19: ReopeningCOVID-19 Resources and Recommendations
Employee Screening Guidance
Building a Safe & Strong Oregon
General Guidelines
Implement workplace safeguards as feasible or when required.
- Consider regular health checks (e.g., temperature and respiratory symptom screening) or symptom self-report of employees, if job-related and consistent with business necessity.
State Questionnaire:
Have you had any of the following COVID-19 symptoms since your last day at work or the last time you were here:
- Fever (100.4F or higher) or chills?
- Cough?
- Shortness of breath or difficulty breathing?
- Fatigue?
- Muscle or body aches?
- Headache?
- New loss of taste or smell?
- Sore throat?
- Congestion or runny nose?
- Nausea or vomiting?
- Diarrhea?
- Persistent pain or pressure in the chest?
- New confusion?
- Inability to wake or stay awake?
- Bluish lips or face?
Process to Reopen Pennsylvania
the commonwealth must ensure there is:
Identification of area’s high-risk settings, including correctional institutions, personal care homes, skilled nursing facilities, and other congregate care settings, and assurance that facilities have adequate safeguards in place such as staff training, employee screening, visitor procedures and screening, and adequate supplies of PPE to support continued operations.
Start for FreeState Questionnaire:
- Fever (100.4F or higher) or chills?
- Cough?
- Shortness of breath or difficulty breathing?
- Fatigue?
- Muscle or body aches?
- Headache?
- New loss of taste or smell?
- Sore throat?
- Congestion or runny nose?
- Nausea or vomiting?
- Diarrhea?
- Persistent pain or pressure in the chest?
- New confusion?
- Inability to wake or stay awake?
- Bluish lips or face?
Additional information:
Process to Reopen PennsylvaniaReopening RI
For ALL Employers:
RIDOH requires establishing, at minimum, symptom screening and COVID-19 risk procedures to screen anyone entering a business or organization’s facilities. People whose responses to screening questions indicate they are sick, or who show visible signs of illness, must be denied entrance and instructed to isolate.
- At a minimum, businesses and organizations must screen employees and visitors for self-reported symptoms consistent with COVID-19 and other COVID-19 risk factors upon entering the building.
- Screenings can be conducted verbally, by app, by phone, or by another method of the employer’s choosing including, if necessary, the posting of an informational poster that communicates the screening requirements.
Additional information:
Reopening RIPhase II General Business and Organization Guidance
Rhode Island Screening Template
State Questionnaire:
Have you had any of the following symptoms in the past three days that are notexplained by allergies or a non-infectious cause?
- Cough?
- Shortness of breath or difficulty breathing?
- Fever
- Chills?
- Muscle Pain?
- Sore throat?
- Headache?
- Nausea or vomiting?
- Diarrhea?
- Runny nose or stuffy nose?
- Fatigue?
- Recent loss of taste or smell?
Have you been in close contact (less than six feet) with anyone with COVID-19 or symptoms of COVID-19 in the past 14 days?
Have you traveled anywhere outside the 50 United States in the past 14 days?
Have you traveled to Rhode Island from another state for a non-work-related purpose in the past 14 days?
Have you been directed to quarantine or isolate by the Rhode Island Department of Health or a healthcare provider in the past 14 days?
Reopening South Carolina
the commonwealth must ensure there is:
DHEC continues to work with federal, state and local partners as it investigates COVID-19 cases in South Carolina. DHEC’s top priority remains protecting the public during this national and state emergency.
Start for FreeState Questionnaire:
- Fever (100.4F or higher) or chills?
- Cough?
- Shortness of breath or difficulty breathing?
- Fatigue?
- Muscle or body aches?
- Headache?
- New loss of taste or smell?
- Sore throat?
- Congestion or runny nose?
- Nausea or vomiting?
- Diarrhea?
- Persistent pain or pressure in the chest?
- New confusion?
- Inability to wake or stay awake?
- Bluish lips or face?
South Dakota's Back to Normal Plan
For ALL Employers:
This guidance is intended for screening of employee prior to the start of the workday. It is not intended for people confirmed or suspected COVID-19, including persons under investigation. Individuals with confirmed or suspected COVID-19 should follow the guidance found here.
Consider implementing a daily health screening check point and log for all employees entering the workplace.
Start for FreeAdditional information:
COVID-19 in South DakotaBack to Normal Plan
Business Screening Guidelines
State Questionnaire:
Askemployees reporting to work the following questions:
Do you have any of the following?
- Fever or chills?
- Cough?
- Shortness of breath or difficulty breathing?
- Fatigue?
- Muscle or body aches?
- Headache?
- New loss of taste or smell?
- Sore throat?
- Congestion or runny nose?
- Nausea or vomiting?
- Diarrhea?
Are you ill, or caring for someone who is ill?
In the two weeks before you felt sick, did you:
- Have contact with someone diagnosed with COVID-19?
- Live in or visit a place where COVID-19 is spreading?
Reopening Tennessee Responsibly
To protect the safety and livelihoods of Tennesseans by operating businesses according to the guidelines and best practices established by the CDDC, state and local government officials in partnership with industry leaders.
For ALL Businessess:
Screen all employees reporting to work for COVID-19 symptoms with the following questions:
- Have you been in close contact with a confirmed case of COVID-19?
- Are you experiencing a cough, shortness of breath or sore throat?
- Have you had a fever in the last 48 hours?
- Have you had new loss of taste or smell?
- Have you had vomiting or diarrhea in the last 24 hours?
State Questionnaire:
- Have you been in close contact with a confirmed case of COVID-19?
- Are you experiencing a cough, shortness of breath or sore throat?
- Have you had a fever in the last 48 hours?
- Have you had new loss of taste or smell?
- Have you had vomiting or diarrhea in the last 24 hours?
Additional information:
Tennessee's COVID-19 ResourcesGeneral Guidelines for Businesses
Start for Free
Opening the State of Texas
On May 18 and May 26, Governor Greg Abbott issued Executive Orders to announce the second phase of the ongoing plan to open additional businesses and activities in Texas. This announcement expands upon the businesses and activities included in the first phase of the plan to Open Texas while minimizing the spread of COVID-19. All newly opened businesses and services are subject to the recommended minimum standard health protocols outlined by DSHS.
ALL Businessess Must:
Screen employees and contractors before coming into the business.
Start for FreeAdditional information:
Opening the State of TexasProtocols for all Employers
State Questionnaire:
Have you had any of the following new or worsening signs or symptoms of possible COVID-19:
- Cough?
- Shortness of breath or difficulty breathing?
- Chills?
- Repeated shaking with chills?
- Muscle pain?
- Headache?
- Sore Throat?
- Loss of taste or smell?
- Diarrhea?
- Feeling feverish or a measured temperated greater than or equal to 100.0 degrees Fahrenheit?
- Known close contact with a person who is lab confirmed to have COVID-19?
If you have been diagnosed with COVID-19:
- Has at least 3 days (72 hours) passed since recovery (resolution of fever without the use of fever-reducing medications)?
- Have you had improvement in symptoms (e.g., cough, shortness of breath)?
- Have at least 10 days passed since symptoms first appeared?
If you have exhibited symptoms that could be COVID-19 and have not been evaluated by a medical professional or tested for COVID-19:
- Are you a healthcare worked or critical infrastructure worker?
- Have you completed a 14 day self-quarantine period form the last date of exposure?
Utah Leads Together
Governor Herbert’s comprehensive task force plan to mitigate the economic consequences of COVID-19.
Best Practices for all Employers:
Those who are, or work with, high-risk populations, should undergo daily screening/symptom monitoring, and be tested if they begin to experience COVID-19 symptoms. High-risk populations should take extra precautions to avoid close contact with multiple people
For Nursing Homes and Long Term Care Facilities:
Primary prevention – Strict visitation policies, screening of staff and visitors, staff must wear PPE for every contact and strive to work at one facility only, and reduced movement of high-risk residents
Additional information:
Utah Leads TogetherBusiness Best Practice Guidelines
State Questionnaire:
Have you had any of the following new or worsening signs or symptoms of possible COVID-19:
- Fever (100.4F or higher) or chills?
- Cough?
- Shortness of breath or difficulty breathing?
- Fatigue?
- Muscle or body aches?
- Headache?
- New loss of taste or smell?
- Sore throat?
- Congestion or runny nose?
- Nausea or vomiting?
- Diarrhea?
- Persistent pain or pressure in the chest?
- New confusion?
- Inability to wake or stay awake?
- Bluish lips or face?
Restart Vermont
MANDATORY HEALTH & SAFETY REQUIREMENTS FOR ALL BUSINESS, NON-PROFIT & GOVERNMENT OPERATIONS
All businesses must follow Vermont Department of Health and CDC Guidelines:
- Prior to the commencement of each work shift, pre-screening and health survey shall be required to verify each employee has no symptoms of respiratory illness (fever, cough, shortness of breath or difficulty breathing, chills, repeated shaking with chills, muscle pain, sore throat, new loss of taste or smell). At the present time non-contact thermometers are in short supply, however employers shall immediately order, and use their best efforts to obtain, thermometers in order to conduct routine temperature checks.
Additional information:
Vermont COVID-19 Recovery Resource CenterStay Home Stay Safe Order
State Questionnaire:
Have you had any of the following new or worsening signs or symptoms of possible COVID-19:
- Fever (100.4F or higher) or chills?
- Cough?
- Shortness of breath or difficulty breathing?
- Fatigue?
- Muscle or body aches?
- Headache?
- New loss of taste or smell?
- Sore throat?
- Congestion or runny nose?
- Nausea or vomiting?
- Diarrhea?
- Persistent pain or pressure in the chest?
- New confusion?
- Inability to wake or stay awake?
- Bluish lips or face?
Forward Virginia
Enhanced Cleaning and Disinfection Best Practices:
Prior to a shift and on days employees are scheduled to work, employers should screen employees prior to starting work. Employees should also self-monitor their symptoms by self-taking of temperature to check for fever and utilizing the questions provided in the VDH Interim Guidance for COVID -19 Daily Screening of Employees before reporting to work. For employers with established occupational health programs, employers can consider measuring temperature and assessing symptoms of employees prior to starting work/before each shift. CDC considers a person to have a fever when he or she has a measured temperature of 100.4° F (38° C) or greater, feels warm to the touch, or gives a history of feeling feverish.
Additional information:
Forward Virginia PlanBusiness Guidelines
Virginia Guidance for Employee Screening
State Questionnaire:
Employees should assess themselves for symptoms of COVID-19 before reporting to work for each shift. Employees should ask themselves: “YES or NO since my last day of work, have I had any of the following:”
- A new fever (100.4°F or higher) or a sense of having a fever?
- A new cough that cannot be attributed to another health condition?
- New shortness of breath or difficulty breathing that cannot be attributed to another health condition?
- New chills that cannot be attributed to another health condition?
- A new sore throat that cannot be attributed to another health condition?
- New muscle aches (myalgia) that cannot be attributed to another health condition or specific activity (such as physical exercise)?
- A new loss of taste or smell?
- Contact with someone in the past 14 days with suspected or confirmed COVID-19?
Washington: Safe Start plans and guidance for reopening
Screen all workers at the beginning of their day by asking them if they have a fever, cough, shortness of breath, fatigue, muscle aches, or new loss of taste or smell.
Start for FreeAdditional information:
Washington State Coronavirus Response (COVID-19)Safe Start Plan
Business Guidance
State Questionnaire:
Have you had any of the following new or worsening signs or symptoms of possible COVID-19:
- Fever (100.4F or higher) or chills?
- Cough?
- Shortness of breath or difficulty breathing?
- Fatigue?
- Muscle or body aches?
- Headache?
- New loss of taste or smell?
- Sore throat?
- Congestion or runny nose?
- Nausea or vomiting?
- Diarrhea?
- Persistent pain or pressure in the chest?
- New confusion?
- Inability to wake or stay awake?
- Bluish lips or face?
Reopening Washington D.C.
Who should be screened?- For most establishments, it is recommended that all employees and staff complete a health screening questionnaire. Depending on your setting and offered services, patrons may be recommended to complete the screening as well.
- Refer to the Phase Two guidance documents for more information about screening recommendations in specific settings .
- The screening should be conducted prior to an individual entering an establishment. For example, an employee would complete the screening prior to the start of each shift.
- The questionnaire may be administered in various formats (e.g., in-person, over the phone, via an automated phone line, electronic survey, etc.).
Additional information:
DC's COVID-19 Response SiteDC's Phase II Guidance
Screening Guidance
State Questionnaire:
Have you been exposed to someone with COVID-19 in the last 14 days?
Have you felt like you had a fever in the past day?
Do you have a new or worsening cough today?
Do you have any of these other symptoms today?
- Shortness of breath or difficulty breathing?
- Fatigue?
- Muscle or body aches?
- Headache?
- New loss of taste or smell?
- Sore throat?
- Congestion or runny nose?
- Nausea or vomiting?
- Diarrhea?
West Virginia Strong - The Comeback
Screen employees: Screen all employees reporting to work daily for COVID-19 symptom
Start for FreeAdditional information:
The Comeback PlanState Questionnaire:
- Have you been in close contact with a confirmed case of COVID-19?
- Are you experiencing a cough, shortness of breath, or sore throat?
- Have you had a fever in the last 48 hours?
- Have you had new loss of taste or smell?
- Have you had vomiting or diarrhea in the last 24 hours?
Reopening Wisconsin
Temperature checks and/or symptom screening: identify and isolate sick people
- Screening employees is recommended for some business sectors. If temperature checks are performed, employees taking temperatures should take precautions. The most protective methods involve maintaining a distance of six feet from others and/or physical barriers to minimize close contact with employees. If you screen employees, follow CDC guidelines.
Additional information:
Reopen GuidelinesGeneral Guidelines
State Questionnaire:
Have you had any of the following COVID-19 symptoms since your last day at work or the last time you were here:
- Fever (100.4F or higher) or chills?
- Cough?
- Shortness of breath or difficulty breathing?
- Fatigue?
- Muscle or body aches?
- Headache?
- New loss of taste or smell?
- Sore throat?
- Congestion or runny nose?
- Nausea or vomiting?
- Diarrhea?
- Persistent pain or pressure in the chest?
- New confusion?
- Inability to wake or stay awake?
- Bluish lips or face?
Reopening Wyoming
The Wyoming Department of Health recommends COVID-19 illness screening questions for businesses to use with employees:
Additional information:
Wyoming's COVID-19 Orders and GuidanceGuidance for Employee Screening from the Wyoming Health Department
Start for Free
State Questionnaire:
Do you currently have any of the following:
- Fever (100.4 Fahrenheit or higher) or feeling feverish?
- Chills?
- A new or worsening cough not caused by another health condition?
- New or worsening shortness of breath or difficulty breathing not caused by another health condition?
- New or worsening fatigue not caused by another health condition?
- New or worsening muscle or body aches not caused by another health condition?
- New or worsening headache that is not normal for you and not caused by another health condition?
- New loss of sense of taste or smell?
- Sore throat?
- Congestion or runny nose?
- Nausea or vomiting?
- Diarrhea?
U.S. State Employee Temperature Screening Requirements
As another preventive measure, many states are requiring businesses to check and record employee body temperatures before allowing them to enter work. Preworkscreen has implemented an optional employee temperature self-report feature that allows you to comply with temperature guidelines for different states. Check the table below to see the specific requirements for your state:
| State | Required | Fever |
|---|---|---|
| Alabama | Recommended | 100.4° |
| Alaska | Not Required | N/A |
| Arizona | Not Required | N/A |
| California | Not Required | N/A |
| Colorado | Required | 100.4° |
| Connecticut | Recommended | 100.4° |
| Delaware | Recommended | 99.5° |
| Florida | Not Required | N/A |
| Georgia | Not Required | N/A |
| Hawaii | Not Required | N/A |
| Idaho | Required | 100.4° |
| Illinois | Recommended | 100.4° |
| Indiana | Recommended | N/A |
| Iowa | Not Required | N/A |
| Kansas | Recommended | 100.4° |
| Kentucky | Required | 100.4° |
| Louisiana | Not Required | N/A |
| Maine | Not Required | N/A |
| Maryland | Recommended | N/A |
| Massachusetts | Not Required | N/A |
| Michigan | Required | 100.4° |
| Minnesota | Recommended | N/A |
| Mississippi | Not Required | N/A |
| Missouri | Not Required | N/A |
| Montana | Not Required | N/A |
| Nebraska | Recommended | N/A |
| Nevada | Not Required | N/A |
| New Hampshire | Required | 100.0° |
| New Jersey | Required | N/A |
| New Mexico | Recommended | 100.4° |
| New York | Recommended | N/A |
| North Carolina | Not Required | N/A |
| North Dakota | Recommended | N/A |
| Ohio | Not Required | N/A |
| Oklahoma | Not Required | N/A |
| Oregon | Recommended | N/A |
| Pennsylvania | Recommended | 100.4° |
| Rhode Island | Not Required | N/A |
| South Carolina | Recommended | N/A |
| South Dakota | Not Required | N/A |
| Tennessee | Recommended | 100.4° |
| Texas | Recommended | 100.0° |
| Utah | Recommended | N/A |
| Vermont | Required | 100.4° |
| Virginia | Recommended | 100.4° |
| Washington | Required | 100.4° |
| West Virginia | Recommended | 100.0° |
| Wisconsin | Not Required | N/A |
| Wyoming | Not Required | N/A |
U.S. State Employee Out-of-State Travel & Quarantine Requirements
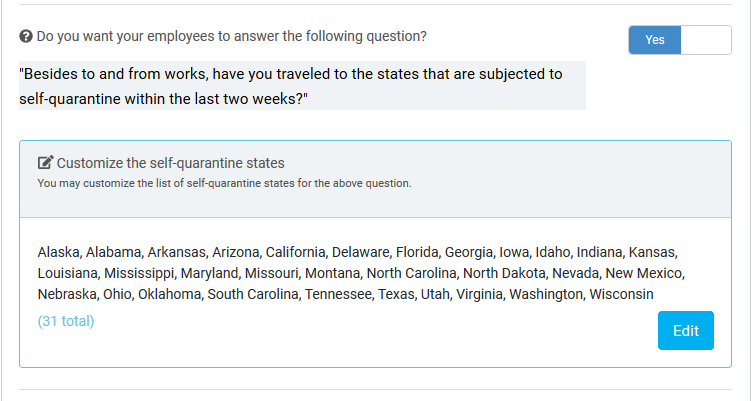
Many states are requiring that employees report out-of-state travel and quarantine for 14 days after their return. Preworkscreen now supports a configurable question that asks employees about recent out-of-state travel and records the places they have visited. When companies choose to use this question, employees will be told to not report to work if they have traveled to states that are considered high-risk for contracting COVID-19 and not completed a 14 day quarantine.
Below, you can find a picture showcasing what the configuration options in the company dashboard for the out-of-state travel question:
Canada Employee Symptom Screening Requirements
State Questionnaire:
1. Are you experiencing any of the following:
- severe difficulty breathing (e.g., struggling for each breath, speaking in single words)?
- severe chese pain?
- having a very hard time waking up?
- feeling confused?
- lost consciousness?
2. Are you experiencing any of the following:
- shortness of breath at rest
- inability to lie down because of difficulty breathing
- chronic health conditions that you are having difficulty managing because of your current respiratory illness
3. In the past 10 days, have you experienced any of the following:
- Fever
- New on set cough or worsening of chronic cough
- New or worsening shortness of breath
- New or worsening difficulty breathing
- Sore throat
- Runny nose
4. Do you have any of the following:
- Chills
- Painful swallowing
- Stuffy nose
- Headache
- Muscle or joint ache
- Feeling unwell, fatigue or severe exhaustion
- Nausea, vomiting, diarrhea or unexplained loss of appetite
- Loss of sense of smell or taste
- Conjunctivitis (pink eye)
5. In the past 14 days, has your employer or AHS told you you’ve been in close contact with a confirmed case of COVID-19?
6. In the past 14 days, did you return from travel outside of Canada?
7. Asymptomatic testing is now only available for specific Albertans. Do you require testing for the purpose of upcoming travel?
State Questionnaire:
1. Are you experiencing any of the following:
- Severe difficulty breathing (e.g. struggling to breathe or speaking in single words)
- Severe chest pain
- Having a very hard time waking up
- Feeling confused
- Losing consciousness
2. Are you experiencing any of the following:
- Mild to moderate shortness of breath
- Inability to lie down because of difficulty breathing
- Chronic health conditions that you are having difficulty managing because of difficulty breathing
3. Are you experiencing cold, flu or COVID-19-like symptoms, even mild ones? Symptoms include: Fever*, chills, cough or worsening of chronic cough, shortness of breath, sore throat, runny nose, loss of sense of smell or taste, headache, fatigue, diarrhea, loss of appetite, nausea and vomiting, muscle aches. While less common, symptoms can also include: stuffy nose, conjunctivitis (pink eye), dizziness, confusion, abdominal pain, skin rashes or discoloration of fingers or toes. Fever: Average normal body temperature taken orally is about 37°C. For more on normal body temperature and fevers, see HealthLinkBC's information for children age 11 and younger and for people age 12 and older.
4. Have you travelled to any countries outside Canada (including the United States) within the last 14 days?
5. Do you provide care or have close contact with a person with confirmed COVID-19? Note: This means you have been contacted by your health authority’s public health team
State Questionnaire:
1. Do you or the person you are inquiring about have any of the following symptoms: severe difficulty breathing (e.g., struggling for each breath, speaking in single words), chest pain, confusion, extreme drowsiness or loss of consciousness?
2. Do you or the person you are inquiring about have shortness of breath at rest or difficulty breathing when lying down?
3. Do you have a new onset of any of the following symptoms?
- fever / chills
- cough
- sore throat / hoarse voice
- shortness of breath
- loss of taste or smell
- vomiting or diarrhea for more than 24 hours
4. Do you have a new onset of 2 or more of any of the following symptoms?
- runny nose
- muscle aches
- fatigue
- conjunctivitis (pink eye)
- headache
- skin rash of unknown cause
- nausea or loss of appetite
- if the patient is an infant, poor feeding
A.1 Have you been in close contact in the last 14 days with someone that is confirmed to have COVID-19?
A.2 Have you had laboratory exposure while working directly with specimens known to contain COVID-19?
A.3 Have you been in a setting in the last 14 days that has been identified by public health as a risk for acquiring COVID-19, such as on a flight, in a workplace or community with a cluster of cases, or at an event?
A.4 Have you received a notification from the COVID Alert app that you may have been exposed to COVID-19?
A.5 Have you travelled outside of Canada, or within Canada excluding travel to western Canada the territories or Ontario west of Terrace Bay in the last 14 days?
A.6 In the last 14 days has anyone living in your household travelled outside of Canada, or within Canada excluding travel to western Canada, the territories or Ontario west of Terrace Bay?
State Questionnaire:
1. Are you experiencing any of the following:
- Severe difficulty breathing (e.g. struggling to breathe or speaking in single words)
- Severe chest pain
- Having a very hard time waking up
- Feeling confused
- Losing consciousness
2. Are you experiencing any of the following:
- Mild to moderate shortness of breath
- Inability to lie down because of difficulty breathing
- Chronic health conditions that you are having difficulty managing because of difficulty breathing
3. Are you experiencing any of the following:
- new or worsening cough
- shortness of breath or difficulty breathing
- temperature equal to or over 38°C
- feeling feverish
- chills
- fatigue or weakness
- muscle or body aches
- new loss of smell or taste
- headache
- gastrointestinal symptoms (abdominal pain, diarrhea, vomiting)
- feeling very unwell
4. Have you travelled to any countries outside Canada (including the United States) within the last 14 days?
5. Within the last 14 days did you provide care or have close contact with a symptomatic person known or suspected to have COVID-19?
A close contact is defined as a person who:
- Provided care for the individual, including healthcare workers, family members or other caregivers, or who had other similar close physical contact without consistent and appropriate use of personal protective equipment; or
- Lived with or otherwise had close prolonged contact (within 2 metres) with the person while they were infectious; or
- Had direct contact with infectious bodily fluids of the person (e.g. was coughed or sneezed on) while not wearing recommended personal protective equipment.
6. Did you have close contact with a person who travelled outside of Canada in the last 14 days who has become ill (new or worsening cough; shortness of breath or difficulty breathing; temperature equal to or over 38°C; feeling feverish; chills; fatigue or weakness; muscle or body aches; new loss of smell or taste; headache; gastrointestinal symptoms (abdominal pain, diarrhea, vomiting); feeling very unwell)?
A close contact is defined as a person who:
- Provided care for the individual, including healthcare workers, family members or other caregivers, or who had other similar close physical contact without consistent and appropriate use of personal protective equipment; or
- Lived with or otherwise had close prolonged contact (within 2 metres) with the person while they were infectious; or
- Had direct contact with infectious bodily fluids of the person (e.g. was coughed or sneezed on) while not wearing recommended personal protective equipment.
State Questionnaire:
1. Are you experiencing any of the following:
- Severe difficulty breathing (e.g. struggling to breathe or speaking in single words)
- Severe chest pain
- Having a very hard time waking up
- Feeling confused
- Losing consciousness
2. Are you experiencing any of the following:
- Mild to moderate shortness of breath
- Inability to lie down because of difficulty breathing
- Chronic health conditions that you are having difficulty managing because of difficulty breathing
3. Are you experiencing 2 or more of the following symptoms (new or worsening)?
- Fever (or signs of a fever such as chills, sweats, muscle aches and lightheadedness)
- Cough
- Headache
- Sore throat
- Painful swallowing
- Runny nose
- Unexplained loss of appetite
- Diarrhea
- Loss of sense of smell or taste
- Or
4. Are you experiencing small red or purple spots on your hands and/or feet?
5. Have you received a notification from the COVID Alert app that you may have been exposed to COVID-19?
6. Are you a resident of an Atlantic province (New Brunswick, Nova Scotia, Prince Edward Island and Newfoundland and Labrador) and traveled outside of these areas within the last 14 days?
7. Are you a resident of a community along the Labrador-Quebec border (Labrador City, Wabush, Fermont, the Labrador Straits area and Blanc Sablon) and traveled outside of these areas in the last 14 days?
8. In the last 14 days, did you have close contact with a person who has been confirmed as having COVID-19?
9. In the last 14 days, did you have close contact with a person who travelled outside of Newfoundland and Labrador who has become ill?
State Questionnaire:
1. Are you experiencing any of the following symptoms:
- difficulty breathing (e.g. unable to finish sentences because of your breathing, short of breath at rest, unable to lie down because of difficulty breathing);
- chest pain;
- having a very hard time waking up;
- fainted or lost consciousness; OR
- difficulty managing your daily life because of breathing difficulties.
2. Are you experiencing ONE of the following symptoms:
- Fever
- New or worsening cough
- Shortness of breath
OR
- TWO of the following symptoms:
- Tiredness
- Generally feeling unwell
- Sore throat
- Muscle aches
- Runny nose
- Headache
- Diarrhea
- Vomiting
- Loss of sense of smell/taste
- Loss of appetite
3. Have you been outside of Canada within the last 14 days?
4. Have you returned to the Northwest Territories from other parts of Canada within the last 14 days (other than Nunavut)?
5. Has anyone in your household been outside of the NWT (other than Nunavut) in the past 14 days?
6. In the last 14 days, have you:
- been in close contact with someone or their respiratory secretions (i.e. saliva and mucous) who is:
- confirmed to have COVID-19; OR
- has COVID-19 symptoms and has had possible exposure to COVID-19 (i.e. travel outside of the NWT in the last 14 days or any points below); OR
- had lab exposure to biological material; OR
- attended a gathering where COVID-19 was spread; OR
- lived or worked in a closed facility experiencing a COVID-19 outbreak.
A close contact is :
- a person who provided care for the person with COVID-19, including family, or other caregivers, and healthcare workers who did not use protective equipment; or
- a person who lived with or otherwise had close contact (within 2 metres) with the person with COVID-19 while they were sick; or
- a person who had direct contact with bodily fluids of someone who has been confirmed to have COVID-19 (e.g. was coughed or sneezed on).
State Questionnaire:
1. Are you experiencing any of the following:
- Severe difficulty breathing (e.g. struggling to breathe or speaking in single words)
- Severe chest pain
- Having a very hard time waking up
- Feeling confused
- Losing consciousness
2. Are you experiencing any of the following:
- Mild to moderate shortness of breath
- Inability to lie down because of difficulty breathing
- Chronic health conditions that you are having difficulty managing because of difficulty breathing
3. Are you experiencing any of the following:
- new or worsening cough
- shortness of breath or difficulty breathing
- temperature equal to or over 38°C
- feeling feverish
- chills
- fatigue or weakness
- muscle or body aches
- new loss of smell or taste
- headache
- gastrointestinal symptoms (abdominal pain, diarrhea, vomiting)
- feeling very unwell
4. Have you travelled to any countries outside Canada (including the United States) within the last 14 days?
5. Within the last 14 days did you provide care or have close contact with a symptomatic person known or suspected to have COVID-19?
A close contact is defined as a person who:
- Provided care for the individual, including healthcare workers, family members or other caregivers, or who had other similar close physical contact without consistent and appropriate use of personal protective equipment; or
- Lived with or otherwise had close prolonged contact (within 2 metres) with the person while they were infectious; or
- Had direct contact with infectious bodily fluids of the person (e.g. was coughed or sneezed on) while not wearing recommended personal protective equipment.
6. Did you have close contact with a person who travelled outside of Canada in the last 14 days who has become ill (new or worsening cough; shortness of breath or difficulty breathing; temperature equal to or over 38°C; feeling feverish; chills; fatigue or weakness; muscle or body aches; new loss of smell or taste; headache; gastrointestinal symptoms (abdominal pain, diarrhea, vomiting); feeling very unwell)?
A close contact is defined as a person who:
- Provided care for the individual, including healthcare workers, family members or other caregivers, or who had other similar close physical contact without consistent and appropriate use of personal protective equipment; or
- Lived with or otherwise had close prolonged contact (within 2 metres) with the person while they were infectious; or
- Had direct contact with infectious bodily fluids of the person (e.g. was coughed or sneezed on) while not wearing recommended personal protective equipment.
State Questionnaire:
1. Do you have any of the following new or worsening symptoms or signs? Symptoms should not be chronic or related to other known causes or conditions.
- Fever or chills
- Difficulty breathing or shortness of breath
- Cough
- Sore throat, trouble swallowing
- Runny nose/stuffy nose or nasal congestion
- Decrease or loss of smell or taste
- Nausea, vomiting, diarrhea, abdominal pain
- Not feeling well, extreme tiredness, sore muscles
2. Have you travelled outside of Canada in the past 14 days?
3. Have you had close contact with a confirmed or probable case of COVID-19?
State Questionnaire:
1. Are you experiencing any of the following:
- Severe pain or tightness in the chest;
- Severe difficulty breathing (i.e. struggling for each breath, speaking in single words);
- Severe abdominal pain;
- Loss of consciousness;
- Prolonged and persistent dizziness or headache;
- An injury that may require stitches or involve a broken bone;
- A child who has prolonged diarrhea or vomiting; or
- A baby under six months of age with a fever of 38C (100.4F) or higher;
2. Do you have any ONE of the following symptoms:
- New or worsening cough;
- Shortness of breath or difficulty breathing;
- Fever;
- Chills;
- Sore Throat;
- Runny nose, sneezing, congestion;
- Headache;
- Muscle aches;
- Unusual fatigue; or
- Acute loss of sense of smell or taste;
State Questionnaire:
1. Are you experiencing any of the following:
- Severe difficulty breathing (e.g. struggling to breathe or speaking in single words)
- Severe chest pain
- Having a very hard time waking up
- Feeling confused
- Losing consciousness
2. Are you experiencing any of the following:
- Mild to moderate shortness of breath
- Inability to lie down because of difficulty breathing
- Chronic health conditions that you are having difficulty managing because of difficulty breathing
3. Are you experiencing any of the following:
- new or worsening cough
- shortness of breath or difficulty breathing
- temperature equal to or over 38°C
- feeling feverish
- chills
- fatigue or weakness
- muscle or body aches
- new loss of smell or taste
- headache
- gastrointestinal symptoms (abdominal pain, diarrhea, vomiting)
- feeling very unwell
4. Have you travelled to any countries outside Canada (including the United States) within the last 14 days?
5. Within the last 14 days did you provide care or have close contact with a symptomatic person known or suspected to have COVID-19?
A close contact is defined as a person who:
- Provided care for the individual, including healthcare workers, family members or other caregivers, or who had other similar close physical contact without consistent and appropriate use of personal protective equipment; or
- Lived with or otherwise had close prolonged contact (within 2 metres) with the person while they were infectious; or
- Had direct contact with infectious bodily fluids of the person (e.g. was coughed or sneezed on) while not wearing recommended personal protective equipment.
6. Did you have close contact with a person who travelled outside of Canada in the last 14 days who has become ill (new or worsening cough; shortness of breath or difficulty breathing; temperature equal to or over 38°C; feeling feverish; chills; fatigue or weakness; muscle or body aches; new loss of smell or taste; headache; gastrointestinal symptoms (abdominal pain, diarrhea, vomiting); feeling very unwell)?
A close contact is defined as a person who:
- Provided care for the individual, including healthcare workers, family members or other caregivers, or who had other similar close physical contact without consistent and appropriate use of personal protective equipment; or
- Lived with or otherwise had close prolonged contact (within 2 metres) with the person while they were infectious; or
- Had direct contact with infectious bodily fluids of the person (e.g. was coughed or sneezed on) while not wearing recommended personal protective equipment.
State Questionnaire:
1. Are you working / volunteering in a Long Term or Continuing Care Home or affiliate facility for any period of time today?
2. Are you working / volunteering in any other SHA facility (not LTC) for any period of time today?
3. Are you experiencing any of the following:
- severe difficulty breathing (e.g., struggling for each breath, speaking in single words)
- severe chest pain
- having a very hard time waking up
- feeling confused
- lost consciousness
4. Are you experiencing any of the following:
- short of breath at rest
- inability to lie down because of difficulty breathing
- chronic health conditions that you are having difficulty managing because of your current respiratory illness
5. Do you have any of the following:
- Fever
- Muscle or joint aches and pains
- Cough
- Loss of sense of smell or taste
- Shortness of breath
- Dizziness
- Sore throat
- Nausea
- Chills
- Vomiting
- Headache
- Diarrhea
- Runny nose
- Loss of appetite (or difficulty feeding for children)
- Conjunctivitis
- Fatigue
- Nasal congestion
6. Were you exposed to someone who is under investigation for COVID-19 or has been confirmed as having COVID-19 within the last 14 days?
7. In the past 14 days have you returned from international travel?
State Questionnaire:
1. Are you experiencing any of the following?
- severe difficulty breathing (for example, struggling for each breath, speaking in single words);
- severe chest pain;
- having a very hard time waking up;
- feeling confused;
- lost consciousness.
2. Are you experiencing any of the following?
- shortness of breath at rest;
- inability to lie down because of difficulty breathing;
- chronic health conditions that you are having difficulty managing because of your current respiratory illness.
3. Do you have any of the following?
- fever/chills
- cough
- shortness of breath
- runny nose
- sore throat
- loss of sense of taste or smell
- headache
- fatigue
- loss of appetite
- nausea or vomiting
- diarrhea
- muscle aches
4. In the past 14 days have you had close contact with someone who is confirmed as having COVID-19?
A close contact is someone who:
- provided care for the individual, including health care workers, family members or other caregivers, or who had other similar close physical contact without consistent and appropriate use of personal protective equipment; or
- who lived with or otherwise had close prolonged contact (within 2 metres) with the person while they were infectious; or
- had direct contact with infectious bodily fluids of the person (such as, was coughed or sneezed on) while not wearing recommended personal protective equipment.
5. In the past 14 days have you returned from travel to any other locations outside of Yukon? Travel includes passing through an airport.